
Change 4 Life Critique
This case study will focus on the C4L campaign, which is an intervention to prevent obesity and part of the 2008 healthy Weight, healthy Lives prevention strategy for England. The £372 million programme includes building cycle lanes, more safe green spaces, and support for early years and pregnancy support. Obesity and its associated noncommunicable diseases are thought to be the biggest threat worldwide; current figures from 2016 state 1.9billion adults were overweight (BMI>25) and 6.5m are obese ( >30) (WHO 2016). If we continue along this trajectory, foresight modelling predicts an increase of 130% obese individuals (Finkelstein et al., 2012). Obesity now causes more deaths than being underweight worldwide (Chan,2017).
Forecasts regarding children are the most concerning, given that children growing up overweight with sedentary lifestyles and poor lifestyle habits are more likely to develop diseases (Sahoo etal.,2015), causing more pressure on the health systems, time off work, therefore impacting economies of the world (Chaker et al.,2015). The UK is ranked 8th for obesity among the adult population which correlates with social class and deprivation: the most deprived 10% are twice as likely to be obese (Coulton et al.,2015). The impact on businesses, society as a whole and the NHS is predicted to cost 49.9 billion (Hausman & Welch, 2010).
Obesity can be viewed as simply as an food energy imbalance (Spiegelman & Flier, 2001), however, the reason for the energy imbalance is multifaceted. The relationship between biology and behaviour is complex and our modern-day obesogenic environment of highly dense, readily available foods and sedentary behaviour does not support healthy human biology. Data has shown the accumulative weight gain overtime affects the whole UK population, especially the most disadvantaged in society and has been coined ‘passive obesity’ (King, 2011).
WHO has set out guidelines to tackle the epidemic for each country to implement. They have advised Governments to create supportive environments to shape better choices of food and activity, making healthy food available and affordable for all (The WHO, 2010). Suggestions include placing a tax on sugary drinks and food, working with food industries to reduce sugar and fat content in processed foods, restrict marketing, especially to children, to implement a worldwide traffic light labelling system, and to support physical activity within schools and the workplace as well as food education and cookery classes (Knai, et al.,2015)
The UK currently has a tier weight management pathway to support obesity. Individuals are supported based on the severity of their needs: from Tier 1 - general health advice; Tier 2 - behaviour and lifestyle change programmes; Tier 3 - specialist intervention and medication; and lastly, gastric band surgery (Maryon-Davis,2005). Interventions to prevent obesity include the Eatwell plate, a reduction in advertisements, low fat, sugar and salt options and education within schools including information and encouragement to sign up to the ‘Change4life campaign’ (C4L) (Department of Health and Social Care, 2020).
The C4L nudge concept created by American academics Richard Thaler and Cass Sunstein was based off Kahneman & Tversky’s (1984) economic model of rational choice. The theory proclaims human rational choice is inconsistent who battle between rational and emotional decision making and are inherently flawed, leaning towards autonomic instant gratification (McDermott,2004). Thaler and Sunstein (2008) state “A nudge is any aspect of behaviour architecture which altars behaviour in a predictable way, without forbidding any options or significantly changing their economic incentives. A nudge must be easy and cheap to avoid.”
Since 2009, David Cameron commissioned psychologist David Halpern and his Behavioural Insights Team in Cabinet Office, now partly privatised, and owned by Nesta, to work on ‘right choices’ public messages, in the form of commercials, educational packages to sign up too, and more recently a sugar swap app (Berger et al.,2019: Goodman et al.,2021). Nudge is primarily to encourage individuals to take responsibility for one’s own health and behaviour (Lehner et al.,2016). The short series of plasticine models, shows a family with working class accents, consuming calorie dense, sugary foods and beverages whilst watching TV or a play on this. The characters are then given an educational tour of the human body, explaining how poor lifestyle choices negatively affect the body, offering suggestions, such as getting outside to exercise, food swaps (since 2015) and eating smaller portions (Department of Health,2011). The messages are aimed at both children and parents, specifically targeted at those families from ethnic minorities and poor socio-economic backgrounds (SES), as well as parents who over feed and use food for short term happiness over long term health, allowing children to choose what they eat, or consume large quantities of snacks (Mulderring, 2018).
The campaign of 26 short clips, logo, website, artwork, and catchy slogans were designed by M&C Saatchi. Sponsors include Kellogg’s, Pepsico, Tesco, Asda, and British Gas. Aardman Animations produced the plasticine characters. The budget was set at £75million. Since 2010, the Government has worked on the campaign being a social movement, backed by businesses rather than central funding, moving it into schools, the NHS, and the voluntary sector to assist the movement and cutting back on expensive advertising.
The campaign’s official figures surpassed its own targets within the first year. The campaign accomplished more than any other UK government campaign and the community have organically transformed the campaign into a collective movement involving volunteer parents, local business support, schools, NHS and mobilised the heart of many communities. The data collected has exceeded marketing targets for signups to the programme and recognition of the logo and plasticine models, but little about the actual long-term data for reducing obesity. The success of the campaign does not correlate to the steadily growing obesity and deprivation figures (see below), now made chronically worse by the COVID 19 Pandemic which has been newly termed “covibesity” (Stavridou et al.,2021).
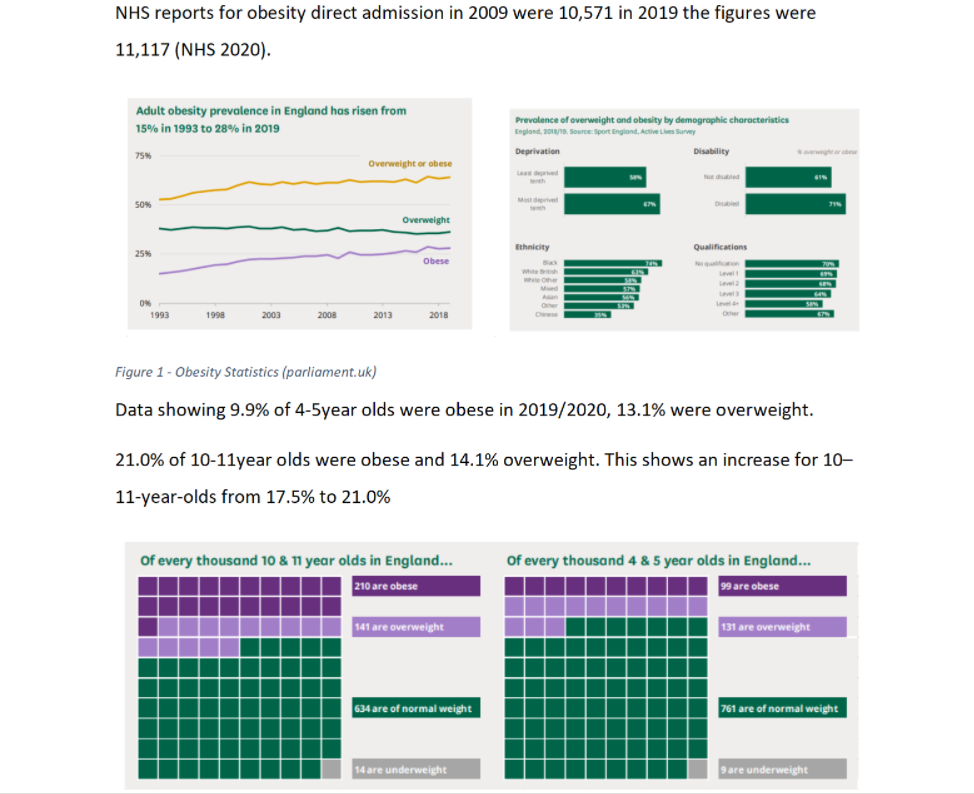
Figure 2 - Obesity Statistics (parliament.uk)
Using subliminal messaging has been a cooperative business tactic since the cold war era: sophisticated branding and marketing is very effective in manipulating emotions to increase sales (Leonard, 2008). The nudge campaign applies this methodology to promote health and well-being to the UK citizens, to reach those most at risk, with the view “Nudging the children of today will lead to a gradual decrease in obesity tomorrow” (Lowenstein, 2017). This ignores the complexity and practicalities of being poor and overlooks the over production of cheap oil with high trans-fat and overly processed foods in the name of capitalism (Mulderring, 2018: Downs et al.,2017). Whilst the campaign is colourful and positive, the reality for the very groups it is targeting is bleak. It fails to address the barriers for low SES and the need for policy change from the very businesses who both supply unhealthy foods and help fund the campaign upstream investment (Mulderrig,2017).
We live in a society where being thin is admired and sought after and being fat is ridiculed (Greenberg et al.,2003). Recently being overweight has become associated with being poor, increased by Cameron’s government blaming the feckless poor who play the system for handouts, not managing their finances, inability to cook and spending their income on fripperies like tattoos (Glaze and Richardson, 2017). This Government view is prevalent in society, blaming obesity on an individual’s poor lifestyle choices rather than a side effect of complex biological interaction with its environment, global capitalism, austerity measures, and a lack of upstream investment (Mollow & McRuer,2015; Glaze & Richardson 2017). Mulderring (2008) states that the campaign seeks to manage the population by governing ‘at a distance’, favouring self-disciplinary control over more coercive forms of state power.
Cameron’s Big Society ideal in reducing reliance on the government and instead relying upon themselves or the local community has escalated and seen the use of food banks replacing adequate social support and allowed the government to avoid its responsibility (Pemberton, 2019). Foodbanks, originally set up for emergency need, are now a controversial business in the UK (Schelling,1984: Hemans, 2021). In 2019, there were 1,200 banks, supplying approximately 1,583, 668 three-day emergency parcels, an 18.8% increase on the year before (Tyler, 2020: Power et al.,2020).); furthermore, the increase in heating and electricity has seen a rise in families choosing between food or heating and the lack of funds to cook food (Begley et al.,2019). There is also still a problem for families accessing healthy food choices in rural areas due to distance and suburban areas where fast food outlets outweigh healthy alternatives in terms of pricing and quantity (Puddephatt et al.,2020). A 2014 study looking into 109 questionnaires completed by minority and low socioeconomic groups (SES) with 58 people currently in receipt of the Healthy Start Vouchers claimed by 80% of those eligible, highlighted that £3.10 per week for pregnant women and children under four and £6.10 for under 1year olds did not correspond positively to the 25% increase in healthy foods or the 12% rise in living costs, furthermore there were complications with shops who accepted them, the application process is difficult and some women weren’t aware they were intitled. For those who used them, they said that they were very valuable and better than receiving cash as it helped to eat fresh fruit and veg (McFadden et al.,2014).
A study researching childhood stereotypes and dietary knowledge, found children under 6 consistently picked out obese characters in a body image line-up of individuals of various sizes as unhealthy, unsuccessful; slim women were constantly viewed as attractive, successful and of value in society. The children were able to pick out most healthy food products, but did struggle to correctly identify unhealthy products, such as mayonnaise (Lipowska & Lipowski,2018). Children receive an estimated 40,000 branded messages per year, with 98% promoting high fat, processed foods. One study found; Children preferred foods packaged in branded containers; a study observed non-McDonald’s food placed in McDonald’s packaging was liked more by children (Keller et al.,2012).
The C4L campaign focused on avoiding using the term obesity and used many positive messages which focused on eating more healthy foods and being active. However, the slogan “eat well, move more, live better” has been criticised (Libbey et al.,2008). Health stigma is on the rise and there is evidence that individuals are not attending vital health screening and check ups for fear of stigma (O’Donoghue, et al.,2021). Governments have the power to raise awareness and education or cause harm (Rubino et al.,2020). Nonetheless a perfect slogan may not exist (Diabetes 2020: Day et al.,2021). A health message study found perceived positive messages such as increase fruit and veg were embraced and acted on, whereas perceived stigmatising or fear based negative messages (including C4L slogan) have a detrimental effect and cause psychological harm. Another study showing 48% of children who fell victim to being teased by both peers and family members, reported fears of losing control of their eating, ate in secret, reported higher level of depression, anxiety and behaviours associated with eating disorders such as binge eating. Similar to other findings (Libbey et al.,2008; Eisenberg et al.,2003; Eisenberg et al.,2006).

A study into sugar swaps Instructed 49 participants to swap high fat / sugar content foods for low fat /sugar alternatives. The families self-reported calories consumed and body composition measurements. The results showed positive improvements from baseline to immediate follow up and one year later that engagement in the change4life sugar swaps reduced consumption of sugar and increased fruit and veg intake. The study did rely on self-reported measures and the calorie intake feedback were unusually low, the trail also paid £300 in vouchers so had limitations and possible biases (Lamport et al.,2022). Another study has shown that the health marketing campaign was effective in reducing sugars by approximately 2% of total energy within a families’ who had shown an interest in previous Change4Life campaigns, however reductions were not maintained when checked 1 year later. The study highlighted the need for clarity of types of sugars to avoid which was attributed to 2.4% increase likely from milk and dairy fat, a case for Clear regulatory guidance for consumers (Bradley et al.,2020).
A 2016 UK diet and Food survey found that the confusing use of language of added sugar and free sugars is adding to the obesity epidemic. In a move to monitor free sugar as opposed to non-milk-extrinsic sugars, the aim was to reduce the UK daily intake to 5%, which was reportedly 10% (the highest contributor was cereals) for 4-11year old, 11% for 11-18 (mostly from non-alcoholic beverages) and 7% (from preserves and confectionery) for adults. The most common free sugar culprits were granulated sugar and glucose syrup from cereals, confectionery, beverages, and milk products. Highlighting the need for clear guidelines again (Amoutzopoulos et al.,.2020).
A study done to view how parents interacted with the C4L material, was disappointing. A third of parents filled out the paperwork, however much of form was used to criticise the patronising material, the target group (low SES) found it both patronising and impractical. No families felt their children’s behaviours needed to change, a high proportion felt their child’s health was adequate and the few who felt the diet could be improved said the cost was a barrier. There were encouraging short term effects in lower SES groups. The C4L raised awareness but did not gain significant material engagement. C4L does now include behaviour change science and consistently evolves (Wrieden & Levy, (2016).
C4L has been heavily criticised, and it is difficult to find supporting evidence of positive impact, however it has a wide reach and has raised awareness (Croker et al.,2012). The Government has taken the approach to tackle obesity from many angles (Gortmaker et al.,2011). there is not a single strategy to fix the problem and will take many polies such as sugar tax, reduction in advertising of unhealthy foods, Reduction of price offers on junk foods, Clarity with nutrient labelling, reduced portion sizes, Improved buying for all, positive messages to raise awareness of reducing sugar and eating for health (Evans, 2017:Marmot et al.,2021). Waxman, (2004) states changes in dietary and physical activity patterns are often the result of environmental and societal changes associated with development and lack of supportive policies in sectors such as health, agriculture, transport, urban planning, environment, food processing, distribution, marketing, and education. A whole societal effort involving health professionals, media, food industry and communities is required. Upstream measures and early intervention into schools is vital (Flynn et al.,). C4L has grown and improved overtime, it now includes phone apps and behaviour change science (Teixeira & Marques, 2017). Whilst it still does not do enough to support the hardest to reach in society thought to need intensive behaviour change (Reicks et al.,2014).. More funding is needed to work with families cooking at home using behaviour change models such as Self-Efficacy Theory (Bandura,1989), Health belief model (Becker,1974) Planned behaviour theory (Ajzen,1991).
C4L does raise awareness through schools, alongside cooking classes and growing vegetables, an increasing activity within primary schools, (Sallis & Glanz, 2009) which may act as a reference point for children from disadvantaged backgrounds to make choices within their control (Ohly etal.,2016). The Government also provide school meals, breakfast clubs and snacks within schools for low SES children, whilst the meals have been notoriously poor in nutritional value and Jamie Oliver has campaigned tirelessly to improve school dinners and raise standards (Belot & James, 2011). C4L is far from perfect, it could improve by changing its slogan and does not address the austerity measures and consequences we will see from increased inflation this year (2022), likely to see increasing families with high levels of debt and limited healthy food choice (Stewart, 2021: Schelling,1984). Although Capitalism is unlikely to stop the foreword momentum. Globally, Governments need to stand up to the food industries and install strict policies and apply levies (Gortmaker et al.,2011). using the money to support community projects to protect and support the most vulnerable and empower the people to change food standards through personal buying power, shunning unethical companies and unhealthy foods which cause harm (Allen & Kovach,2000)
References
Ajzen, I. (2011). The theory of planned behaviour: Reactions and reflections. Psychology & health, 26(9), 1113-1127.
Allen, P., & Kovach, M. (2000). The capitalist composition of organic: The potential of markets in fulfilling the promise of organic agriculture. Agriculture and human values, 17(3), 221-232.Bandura, A. (1989). Human agency in social cognitive theory. American psychologist, 44(9), 1175.
Amoutzopoulos, B., Steer, T., Roberts, C., Collins, D., & Page, P. (2020). Free and added sugar consumption and adherence to guidelines: the UK National Diet and Nutrition Survey (2014/15–2015/16). Nutrients, 12(2), 393.
Becker, M. H. (1974). The health belief model and sick role behavior. Health education monographs, 2(4), 409-419.
Begley, A., Paynter, E., Butcher, L. M., & Dhaliwal, S. S. (2019). Examining the association between food literacy and food insecurity. Nutrients, 11(2), 445.
Berger, N., Cummins, S., Smith, R. D., & Cornelsen, L. (2019). Recent trends in energy and nutrient content of take-home food and beverage purchases in Great Britain: an analysis of 225 million food and beverage purchases over 6 years. BMJ nutrition, prevention & health, 2(2), 63.
Birch, L. L., & Davison, K. K. (2001). Family environmental factors influencing the developing behavioral controls of food intake and childhood overweight. Pediatric Clinics, 48(4), 893-907.
Bradley, J., Gardner, G., Rowland, M. K., Fay, M., Mann, K., Holmes, R., ... & Moynihan, P. (2020). Impact of a health marketing campaign on sugars intake by children aged 5–11 years and parental views on reducing children’s consumption. BMC public health, 20(1), 1-11.
Briggs, S., & Foord, M. (2017). Food Banks and the Transformation of British Social Welfare. Czech & Slovak Social Work/Sociální Práce/Sociálna Práca, 17(4).
Brookes, G., & Harvey, K. (2015). Peddling a semiotics of fear: a critical examination of scare tactics and commercial strategies in public health promotion. Social Semiotics, 25(1), 57-80.
Chaker, L., Falla, A., van der Lee, S. J., Muka, T., Imo, D., Jaspers, L., ... & Franco, O. H. (2015). The global impact of non-communicable diseases on macro-economic productivity: a systematic review. European journal of epidemiology, 30(5), 357-395.
Chan, M. (2017). Obesity and diabetes: The slow‐motion disaster. The Milbank Quarterly, 95(1), 11.
Cleland, V., Nash, M., Sharman, M. J., & Claflin, S. (2019). Exploring the health-promoting potential of the “parkrun” phenomenon: what factors are associated with higher levels of participation? American Journal of Health Promotion, 33(1), 13-23.
Coulton, V., Dodhia, S., Ells, L., Blackshaw, J., & Tedstone, A. (2015). National mapping of weight management services:: provision of tier 2 and tier 3 services in England.
Croker, H., Lucas, R., & Wardle, J. (2012). Cluster-randomised trial to evaluate the ‘Change for Life’mass media/social marketing campaign in the UK. BMC Public Health, 12(1), 1-14.
Day, R., Bridge, G., Austin, K., Ensaff, H., & Christian, M. (2021). Parents’ awareness and perceptions of the Change4Life 100 calorie snack campaign, and perceived impact on snack consumption by children under 11 years.
Department of Health and Social Care. (2020). Tackling obesity: empowering adults and children to live healthier lives.
Department of Health. (2011). Change4Life Three Year Social Marketing Strategy.
Diabetes, T. L. (2020). Obesity-related stigma—hiding in plain sight. The lancet. Diabetes & endocrinology, 8(5), 349.
Downs, S. M., Bloem, M. Z., Zheng, M., Catterall, E., Thomas, B., Veerman, L., & Wu, J. H. (2017). The impact of policies to reduce trans fat consumption: a systematic review of the evidence. Current developments in nutrition, 1(12), cdn-117.
Eisenberg, M. E., Neumark-Sztainer, D., & Story, M. (2003). Associations of weight-based teasing and emotional well-being among adolescents. Archives of pediatrics & adolescent medicine, 157(8), 733-738.
Eisenberg, M. E., Neumark-Sztainer, D., Haines, J., & Wall, M. (2006). Weight-teasing and emotional well-being in adolescents: Longitudinal findings from Project EAT. Journal of adolescent health, 38(6), 675-683.
Evans, C. E. L. (2017). Sugars and health: a review of current evidence and future policy. Proceedings of the Nutrition Society, 76(3), 400-407.
Finkelstein, E. A., Khavjou, O. A., Thompson, H., Trogdon, J. G., Pan, L., Sherry, B., & Dietz, W. (2012). Obesity and severe obesity forecasts through 2030. American journal of preventive medicine, 42(6), 563-570.
Flynn, M. A. T., McNeil, D. A., Maloff, B., Mutasingwa, D., Wu, M., Ford, C., & Tough, S. C. (2006). Reducing obesity and related chronic disease risk in children and youth: a synthesis of evidence with ‘best practice’recommendations. Obesity reviews, 7, 7-66.
Glaze, S., & Richardson, B. (2017). Poor choice? Smith, Hayek and the moral economy of food consumption. Economy and Society, 46(1), 128-151.
Goodman, S., Armendariz, G., Corkum, A., Arellano, L., Jáuregui, A., Keeble, M., ... & Hammond, D. (2021). Recall of government healthy eating campaigns by consumers in five countries. Public Health Nutrition, 1-31.
Gortmaker, S. L., Swinburn, B. A., Levy, D., Carter, R., Mabry, P. L., Finegood, D. T., ... & Moodie, M. L. (2011). Changing the future of obesity: science, policy, and action. The Lancet, 378(9793), 838-847.
Gortmaker, S. L., Swinburn, B. A., Levy, D., Carter, R., Mabry, P. L., Finegood, D. T., ... & Moodie, M. L. (2011). Obesity 4 Changing the future of obesity: science, policy, and action. Lancet, 378, 838-47.
Greenberg, B. S., Eastin, M., Hofschire, L., Lachlan, K., & Brownell, K. D. (2003). Portrayals of overweight and obese individuals on commercial television. American journal of public health, 93(8), 1342-1348.
Hemans, E. (2021). Aligning Local Interventions with the UN Sustainable Developments Goals (SDGs).
Keller, K. L., Kuilema, L. G., Lee, N., Yoon, J., Mascaro, B., Combes, A. L., ... & Halford, J. C. (2012). The impact of food branding on children's eating behavior and obesity. Physiology & behavior, 106(3), 379-386.
King, D. (2011). The future challenge of obesity. The Lancet, 378(9793), 743-744.
Kite, J., Grunseit, A., Bohn-Goldbaum, E., Bellew, B., Carroll, T., & Bauman, A. (2018). A systematic search and review of adult-targeted overweight and obesity prevention mass media campaigns and their evaluation: 2000–2017. Journal of health communication, 23(2), 207-232.
Knai, C., Petticrew, M., Durand, M. A., Eastmure, E., James, L., Mehrotra, A., ... & Mays, N. (2015). Has a public–private partnership resulted in action on healthier diets in England? An analysis of the Public Health Responsibility Deal food pledges. Food policy, 54, 1-10.
Lamport, D. J., Wu, S. Y., Drever-Heaps, J., Hugueniot, O., Jones, D. J., Kennedy, O. B., ... & Butler, L. T. (2022). Can Public Health Interventions Change Immediate and Long-Term Dietary Behaviours? Encouraging Evidence from a Pilot Study of the UK Change4Life Sugar Swaps Campaign. Nutrients, 14(1), 68.
Lehner, M., Mont, O., & Heiskanen, E. (2016). Nudging–A promising tool for sustainable consumption behaviour?. Journal of Cleaner Production, 134, 166-177.
Leonard, T. C. (2008). Richard H. Thaler, Cass R. Sunstein, Nudge: Improving decisions about health, wealth, and happiness.
Leonard, T.C., Goldfarb, R. S., & Suranovic, S.M. (2000). New on paternalism and Public Policy. Economics and Philosophy, 16, 323-331.
Libbey, H. P., Story, M. T., Neumark‐Sztainer, D. R., & Boutelle, K. N. (2008). Teasing, disordered eating behaviors, and psychological morbidities among overweight adolescents. Obesity, 16(S2), S24-S29.
Lipowska, M., & Lipowski, M. (2018). Children’s Awareness of Healthy Behaviours—Validity of Beauty & Health and Dietary Knowledge & Habits Scales. Health Psychol. Rep, 6.
Lowenstein, G., & Charter, N. (2017). Putting nudges in perspective.
Marmot, M., Allen, J., Goldblatt, P., Herd, E., & Morrison, J. (2021). Build back fairer: the COVID-19 Marmot review the pandemic, socioeconomic and health inequalities in England.
Maryon-Davis, A. (2005). Weight management in primary care: how can it be made more effective?. Proceedings of the Nutrition Society, 64(1), 97-103.
McDermott, R. (2004). The feeling of rationality: The meaning of neuroscientific advances for political science. Perspectives on politics, 2(4), 691-706.
McFadden, A., Green, J. M., Williams, V., McLeish, J., McCormick, F., Fox-Rushby, J., & Renfrew, M. J. (2014). Can food vouchers improve nutrition and reduce health inequalities in low-income mothers and young children: a multi-method evaluation of the experiences of beneficiaries and practitioners of the Healthy Start programme in England. BMC public health, 14(1), 1-13.
Mollow, A., & McRuer, R. (2015). Fattening Austerity. Body Politics, 3(5), 25-49.
Mulderrig, J. (2017). Nudge and the politics of wellbeing: bringing biopower into dialogue with critical discourse analysis. Médiation et Information.
Mulderrig, J. (2018). Multimodal strategies of emotional governance: A critical analysis of ‘nudge’tactics in health policy. Critical Discourse Studies, 15(1), 39-67.
Mulderrig, J. (2018). Multimodal strategies of emotional governance: A critical analysis of ‘nudge’tactics in health policy. Critical Discourse Studies, 15(1), 39-67.
O’Donoghue, G., Cunningham, C., King, M., O’Keefe, C., Rofaeil, A., & McMahon, S. (2021). A qualitative exploration of obesity bias and stigma in Irish healthcare; the patients’ voice. PloS one, 16(11), e0260075.
Ohly, H., Gentry, S., Wigglesworth, R., Bethel, A., Lovell, R., & Garside, R. (2016). A systematic review of the health and well-being impacts of school gardening: synthesis of quantitative and qualitative evidence. BMC Public Health, 16(1), 1-36.
Pemberton, C. S. C. (2019). Between Ecclesiology and Ontology: A Response to Chris Allen on British Food Banks. Political Theology, 20(1).
Power, M., Doherty, B., Pybus, K., & Pickett, K. (2020). How COVID-19 has exposed inequalities in the UK food system: The case of UK food and poverty. Emerald Open Research, 2.
Puddephatt, J. A., Keenan, G. S., Fielden, A., Reaves, D. L., Halford, J. C., & Hardman, C. A. (2020). ‘Eating to survive’: A qualitative analysis of factors influencing food choice and eating behaviour in a food-insecure population. Appetite, 147, 104547.
Puhl, R., Peterson, J. L., & Luedicke, J. (2013). Fighting obesity or obese persons? Public perceptions of obesity-related health messages. International Journal of Obesity, 37(6), 774–782. https://doi.org/10.1038/ijo.2012.156
Reicks, M., Trofholz, A. C., Stang, J. S., & Laska, M. N. (2014). Impact of cooking and home food preparation interventions among adults: outcomes and implications for future programs. Journal of nutrition education and behavior, 46(4), 259-276.
Saeedi, P., Petersohn, I., Salpea, P., Malanda, B., Karuranga, S., Unwin, N., ... & IDF Diabetes Atlas Committee. (2019). Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas. Diabetes research and clinical practice, 157, 107843.
Sahoo, K., Sahoo, B., Choudhury, A. K., Sofi, N. Y., Kumar, R., & Bhadoria, A. S. (2015). Childhood obesity: causes and consequences. Journal of family medicine and primary care, 4(2), 187.
Sallis, J. F., & Glanz, K. (2009). Physical activity and food environments: solutions to the obesity epidemic. The Milbank Quarterly, 87(1), 123-154.
Schelling, T. C. (1984). Choice and consequence. Harvard University Press.
Schelling, T. C. (1984). Choice and consequence. Harvard University Press.
Snuggs, S., Houston-Price, C., & Harvey, K. (2019). Healthy eating interventions delivered in the family home: A systematic review. Appetite, 140, 114-133.
Spiegelman, B. M., & Flier, J. S. (2001). Obesity and the regulation of energy balance. cell, 104(4), 531-543.
Statistics on Obesity, Physical Activity and Diet 2020: Data tables - NHS Digital
Stavridou, A., Kapsali, E., Panagouli, E., Thirios, A., Polychronis, K., Bacopoulou, F., ... & Tsitsika, A. (2021). Obesity in Children and Adolescents during COVID-19 Pandemic. Children, 8(2), 135.
Stewart, I. (2021). Cold, Hungry And Stressed.
Teixeira, P. J., & Marques, M. M. (2017). Health behavior change for obesity management. Obesity facts, 10(6), 666-673.
Thaler, R. H., & Sunstein, C. R. (2008). Nudge: improving decisions about health. Wealth, and Happiness, 6, 14-38.
Tyler, G. (2020). Food banks in the UK.
Waxman, A. (2004). WHO global strategy on diet, physical activity and health. Food and nutrition bulletin, 25(3), 292-302.
World Health Organization. (2010). Set of recommendations on the marketing of foods and non-alcoholic beverages to children
World Health Organization. (2016). Report of the commission on ending childhood obesity. World Health Organization.
Wrieden, W. L., & Levy, L. B. (2016). ‘Change4Life Smart Swaps’: quasi-experimental evaluation of a natural experiment. Public health nutrition, 19(13), 2388-2392.