
Barriers and Adherence to Exercise

Adherence to exercise is defined by a client’s attendance to set exercise goals for an agreed amount of time. Sustained exercise participation for sedentary individuals depends on many factors. The complex setting and support needed to prevent the statistics of 50% drop out within 3-6 months and even more at 12 months is vital to improve current drop out figures. (Martin, & Dubbert, 1985).
Research has highlighted three main areas which are:
· Outcome expectations
· Self-efficacy
· Social Influences
· Perceptions of control.
What is self-efficacy and why is it important in adherence to exercise? Research suggests by improving self-efficacy and outcome expectations it can increase the likelihood of adhering to an exercise programme (Shaughnessy, et al.,2006;Resnick et al.,2000).
Older adults and Younger adults tend to exercise for different rewards. Older adults have been found to exercise for:
Pleasure
Social enjoyment
Pain / condition improvement
Weight loss
Younger adults for:
Challenge /competitions
Fitness goals
There are many theories to draw from when supporting individuals with the adherence to exercise. Popular models are:
Health belief model
Theories of reason, action and planned behaviour
Self-efficacy Theory
Locus of control, self-determination Theory
(Biddle & Nigg,2000).
A study was done on 312 stroke survivors to assess Self-efficacy and the relationship to adherence of a rehab programme.
In stroke victims the most common barriers to exercise were:
Fear of failing
Accessing exercise venues
High costs
Transport issues
Fatigue
Lack of motivation
Lack of partner
Depressive symptoms
Motor impairments
The study concluded that intervention to strengthen adherence to exercise in the form of reminders from clinicians improve exercise motivation and adherence. It also highlighted a need for better understanding of psychological factors that effect adherence to exercise and self- efficacy. (Almutary & Tayyib, 2020).

Case study:
Comparing the effectiveness of mobile video-guided home exercise programme and standard paper-based home exercise programme.
The study involved stroke victims in Hong Kong adhering to a functional exercise home plan using either a video demonstration or a paper description. The study found that video demonstration was superior to paper instructions for recovering stroke patients adhering to a homebased rehabilitation programme. Also, the study found a strong correlation between SEE (self-efficacy) and adherence during the 3 month follow up period, suggesting that a higher self-efficacy supports persistence in maintaining a programme to achieve the desired outcome. The suggestion that patients found the video demonstrations superior for adherence could be due to clearer visual demonstrations (as opposed to written instructions) leading to the self-belief that the client can replicate the movements themselves (SEE). The research did have limitations such as only studying Chinese patients. A broad range of cultures including countries with different beliefs around rehabilitation and exercise would be advantageous to test the self-efficacy theory (Chung et al.,2020)

The stages of change model.
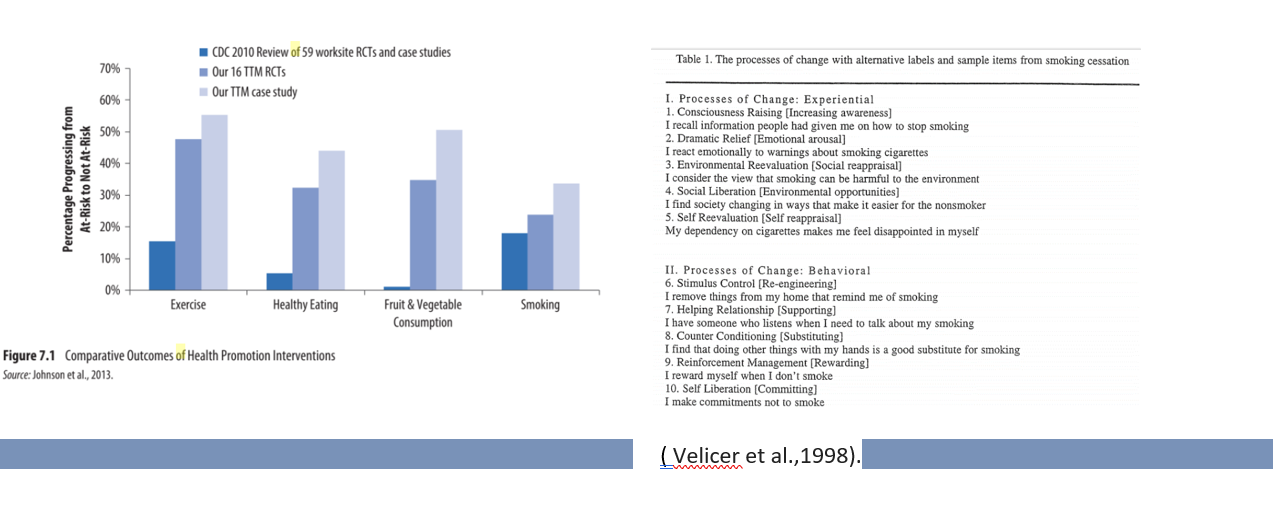
This theory was developed by Prochaska and DiClemente in the late 1970s. The TTM is based on the six stages of behaviour change :(originally habitual /addictive) precontemplation, contemplation, preparation, action, maintenance, and termination. This is not a theory but a model which was discovered through applied research studies of 25 other leading psychotherapy theories, which suggested why people changed behavior. The TTM model explains how people change. The model has allowed leaders in the field to make mathematical equations to predict an individual’s success in behavior change, based on where they are within the model; as well as what needs to change by how much in order to move into the next stage i.e., to move from precontemplation to action would take 15 points of pros of changing.
For example, if an individual lives a sedentary lifestyle, with a business which requires being on the computer all day, (their barrier to exercise) the applied research has found that double the number of benefits would be needed to overpower the barrier. The model has been tested many times and has been found that change of behavior success is more likely if an individual uses all stages of the model along with increasing self-efficacy and intrinsic motivation which is shown much more powerful than extrinsic motivation. (Prochaskaet al., 2015;Velicer et al., 1998).
The health belief model.
This model was developed in the 1950’s by a group of American Psychologists, initially to predict failure in adhering to health changes which may save their lives. It has since been adopted to predict behavior in exercise and eating habits. One piece of research showed that individuals who did not believe they will be at risk if they do not change or believe the benefits associated with health changes (perceived susceptibility), showed a 79% reduction in voluntary Xray screening for Tuberculosis. Four out of five people who did have perceived susceptibility did have the screening.
The six constructs are:
Perceived severity / seriousness: This will include weighing up a variety of factors i.e. if left will the individual decline further, have higher pain levels, need care and support? Social consequences such as will it impact on family, work and wider social commitments?.
Perceived control: Does the individual feel they can influence and make a difference in their lives.
Perceived Benefits: Does the required effort offset with enough gains and benefits. What is important to one individual may be very different to another, so this model will need to be individualized.
Perceived Barriers/cost: possible feelings may include: feeling self-conscious, imagining humiliation, projections that other exercisers are more capable, look better and feel comfortable in an exercise environment. Whereas they may feel that they are incapable, do not look great and feel uncomfortable in an exercise environment. Other barriers include the cost, accessibility, pain and health conditions side effects and fears and, a lack of friends to accompany them.
(Extended) Cues to action: education from as health professional, cues and prompts in the form of text reminders, advertising etc.
Self-efficacy: The belief that with practice the individual can acquire the skills needed and the has determination to see it through.
Modifying factors /Demographic variables: Social psychological variables include the individual’s environment, relationships, upbringing, beliefs and, peers will affect each construct. (Strecher,1997).



References
Ağıl, A., Abıke, F., Daşkapan, A., Alaca, R., & Tüzün, H. (2010). Short-term exercise approaches on menopausal symptoms, psychological health, and quality of life in postmenopausal women. Obstetrics and gynecology international, 2010.
Almutary, H., & Tayyib, N. (2020). Factors associated with exercise self-efficacy among people with chronic diseases. Applied Nursing Research, 54. https://doi.org/10.1016/j.apnr.2020.151275
Bandura, A. (1981). Self-referent thought: A developmental analysis of self-efficacy. Social cognitive development: Frontiers and possible futures, 200(1), 239.
Biddle, S. J., & Nigg, C. R. (2000). Theories of exercise behavior. International Journal of Sport Psychology, 31(2), 290-304.
Chung, B. P. H., Chiang, W. K. H., Lau, H., Lau, T. F. O., Lai, C. W. K., Sit, C. S. Y., ... & Lee, J. S. W. (2020). Pilot study on comparisons between the effectiveness of mobile video-guided and paper-based home exercise programs on improving exercise adherence, self-efficacy for exercise and functional outcomes of patients with stroke with 3-month follow-up: A single-blind randomized controlled trial. Hong Kong Physiotherapy Journal, 40(01), 63-73.
Ebben, W., & Brudzynski, L. (2008). Motivations and barriers to exercise among college students. Journal of Exercise Physiology Online, 11(5).
Fox, K. R. (1999). The influence of physical activity on mental well-being. Public health nutrition, 2(3a), 411-418.
Kemmler, W., Lauber, D., Weineck, J., Hensen, J., Kalender, W., & Engelke, K. (2004). Benefits of 2 years of intense exercise on bone density, physical fitness, and blood lipids in early postmenopausal osteopenic women: results of the Erlangen Fitness Osteoporosis Prevention Study (EFOPS). Archives of Internal Medicine, 164(10), 1084-1091.
Lees, F. D., Clark, P. G., Nigg, C. R., & Newman, P. (2005). Barriers to exercise behavior among older adults: a focus-group study. Journal of aging and physical activity, 13(1), 23-33.
Martin, J. E., & Dubbert, P. M. (1985). Adherence to exercise. Exercise and sport sciences reviews, 13(1), 137-168.
Martinsen, E. W. (1990). Benefits of exercise for the treatment of depression. Sports Medicine, 9(6), 380-389.
Nystoriak, M. A., & Bhatnagar, A. (2018). Cardiovascular effects and benefits of exercise. Frontiers in cardiovascular medicine, 5, 135.
Prochaska, J. O., Redding, C. A., & Evers, K. E. (2015). The transtheoretical model and stages of change. Health behavior: Theory, research, and practice, 97. Page 125-144.
Resnick, B., Palmer, M.H., Jenkins, L.S. and Spellbring, A.M., 2000. Path analysis of efficacy expectations and exercise behaviour in older adults. Journal of advanced nursing, 31(6), pp.1309-1315.
Schunk, D. H., & Pajares, F. (2009). Self-efficacy theory. Handbook of motivation at school, 35-53.
Shaughnessy, M., Resnick, B. M., & Macko, R. F. (2006). Testing a model of post‐stroke exercise behavior. Rehabilitation nursing, 31(1), 15-21.
Stone, G. A. (2018). The neuroscience of self-efficacy: vertically integrated leisure theory and its implications for theory-based programming. Journal of Outdoor Recreation, Education, and Leadership, 10(2).
Strecher, V. J., & Rosenstock, I. M. (1997). The health belief model. Cambridge handbook of psychology, health and medicine, 113, 117.
Sutton, S. (2005). Stage theories of health behaviour. Predicting health behaviour: Research and practice with social cognition models, 2, 223-275.
Velicer, W. F., Prochaska, J. O., Fava, J. L., Norman, G. J., & Redding, C. A. (1998). Smoking cessation and stress management: applications of the transtheoretical model. Homeostasis, 38(5-6), 216-33.