
Bodywork: Injuries, Pain, Weak Muscles and Rehab.
Muscle pain and weakness associated possible physical and emotional symptoms / causations and rehab exercise to support.
The neck
Anterior neck flexors and Posterior neck extensors: Stomach Meridian.
Physical - Stiff neck, whiplash injuries, riding, rugby and football (contact sport), allergies.
Emotions - -distress, needing validation, empathy.
Exercises: Chin tucks, resistance band isometric side flexion, cervical extension.
Levator Scapulae: Stomach Meridian
Physical: Restrictive, hurts to turn, digestive issues, too much acid.
Emotions: emotional upset, dismay
Exercises: shoulder shrugs, Barbell: hang, snatch pull, Overhead single arm dumbbell carry.
Shoulder group.
Teres Major - Governing Meridian
Physical: Acid / Alkali imbalance, Headaches fogginess.
Emotional: Feeling over burdened, trapped emotions.
Exercises: medicine ball slams, lat pull downs, wide press up, YTWL exercises.
Supraspinatus: Central Brain Meridian
Physical - Concentration, driving long distances, brain fatigue, shoulder pain, circular thoughts.
Emotional - Anxiety and emotional distress
Exercises: Shoulder press, resistance band upright row.
Subclavius: Stomach meridian
Weak Rotator cuff muscles
Difficulty lifting arm
Exercises: Alternating floor press
Anterior Serratus- Lung meridian- linked to Deltoid and Diaphragm
Physical: limited shoulder extension, shoulder and rib restriction, Hay fever, coughs, Bronchitis
Exercises: Plank, push up, stir the pot on stability ball, Superman, plank with one arm weighted row.
Subscapularis: Heart meridian
Physical - Elbow problems
Exercises: Resisted dynamic hugs, Gym ball, wall bounces, shoulder horizontal rotations
Deltoids: Lung meridian
Physical - Coughs, bronchitis, difficulty with shoulder extension
Exercises once mobility is restored: Overhead press, Kettle bell lateral raise, Kettle bell frontal raise, kettle bell alternating arm swings
Upper Trapezius: kidney meridian
Physical - Eye and ear problems, weak lats, conjunctivitis, dizzy, glue ear.
Exercises: Strengthen lower trapezius and lats. YTWL exercises, Kettle bell high pull, Hang snatch pull, resisted high row to low row with lateral lunge (TRX)
Pec Minor: Stomach meridian
Physical - Restricted Lymph flow, Shoulder issues, Winged Scapula, anaemia, shallow breathing
Exercises: Barbell bench press, TRX plank
Lower Traps: Spleen Meridian
Physical - desk jobs, frequent coughs, colds, anaemia , tight chest muscles, short arm swing.
Strengthen lower Trapezius, lengthen front line - pecs, anterior neck muscles, belly breath, use a ball to trigger point upper traps and lats.
Infraspinatus: Triple Warmer Meridian - Thymus
linked to teres minor
frequent infections
Emotional: self-esteem / self worth, self doubt
Rhomboids - Liver Meridian
Aching, soreness between shoulder blades
Toxicity of the liver
cross / irritable
seeing floating spots
Latissimus Doris: Spleen /Pancreas Meridian
Weakness, allows the shoulders to raise. High sugar intake
Exercises: Commando crawling, Resisted high row, to low row with lateral lunge, Lat pull down.
Back pain, weakness and associated muscles
Glutes Medius: Circulatory Sex Meridian
Physical - prevents swaying, short stride, PMS, Endometriosis
Emotional: Stress
Exercises - Lunge curtsy, squat jump into explosive jumping jacks, side lunge with medicine ball, narrow lunge.
Sartorius: Triple warmer meridian - adrenals
Physical: knee pain, low blood sugar, ME,
Emotional: Shock, stress
Piriformis - Circulatory Sex Meridian
If bilaterally weak: Jaw issues.
Exercises - Squat with resistance band, resisted abduction with band, resisted clam shell.
Hamstrings: lung Meridian - linked to Sacrum
Physical - Constipation, toxicity of liver, lower bowel toxicity, colitis, restless fatigue, Lower back pain, headaches
emotional - stress, lack of stamina, shallow breathing.
Belly breath to massage organs, eat a whole food diet.
Exercise - Nordic curl, stiff leg dead lift, single leg with dumbbell, bridge single leg on step.
Iliacus: Assists psoas - Kidney Meridian
physical - Water balance, issues with Ileo-Caecal Valve, slow lymph chyme process, IBS, causing back ache, headaches, hip, shoulder, elbow pain.
Exercises - Mountain climbers, reverse lunge with high knee lift, agility acceleration, deceleration.
Psoas: Kidney Meridian
Physical: maintains lumbar spine curve, bilaterally tight leads to lordosis, unilateral results in an uneven pelvis. Bilaterally weak leads to flatback and foot problems and back pain.
Dehydration, kidney imbalances, skin conditions,
Emotions: Fears
Quadratus Lumborum: Large Intestine
Physical - Scoliosis, Pelvis instability, difficulty side bending, constipation, Bowel Issues, Too much bran, try replacing with vegetables and rye.
Exercises - Side plank with trunk rotation, side crunch on half ball, lateral pelvic tilt reaching.
Adductors: Circulatory sex Meridian
Hormones, menopause, cystitis, elbow and shoulder discomfort
Exercises: lunges lateral, lunge lateral with dumbbells, stability ball v splits
Glute Maximus: Circulatory Sex Meridian
Physical - stabilises back,
If bilaterally weak: sway back or lordosis.
Exercises:- Pistol squat, box jumps, lunge curtsy, reverse lunge to explosive hop
Gracilis: Triple Warmer Meridian
Physical: Back ache, knee problems, low blood sugars, hypoglycaemia, allergies, ME
Emotionally - Stress
Exercises: Active hip adduction, As per adductors.
Tensor Fascia Lata: Large intestine Meridian
Physical - supports flexion of the hip, constipation, Colic, Digestion, Back pain, Skin issues, flora imbalance.
Exercises: Lateral leg raise, resisted squat, Isometric hip abduction
Tibialis Anterior / Posterior: Bladder Meridian
Physical - Shin splints, Plantar Fascia, Flat feet, Fallen arches, weak ankles
Emotionally - Adrenal fatigue, exhaustion
Exercises: Heel walks, resisted Dorsi Flexion, Squat on BOSU
Soleus: Triple Warmer - Adrenals
Physical - Difficulty standing on toes, Achilles rupture
Exercises - Bridge with heel raise, Calf raise, ankle bounding
Gastrocnemius: Triple Warmer
Physical - Stabilises foot, Sway back knees, Plantar Fascia
Exercises - Heel raise sitting on wall, mini squat heel raise
A bone break:
Bone is made up of 70% Calcium phosphate proteins and collagen, 20 % organic matrix containing type I collagen fibres and less than 5% of water and lipids.
Proteins influence bone healing restoring it to its original properties.
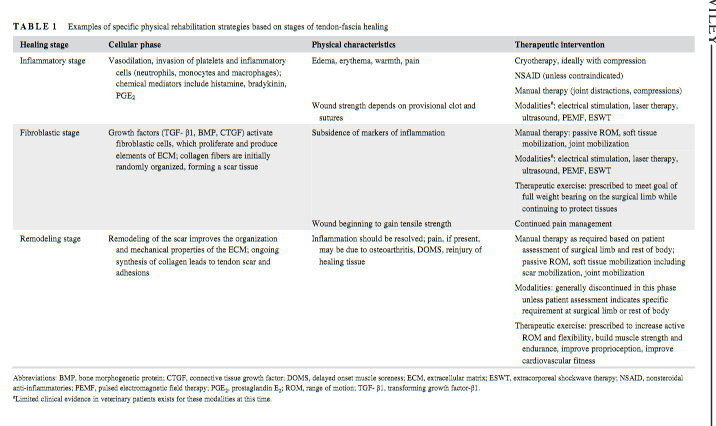
Healing occurs in three overlapping stages:
1) the early inflammatory stage.
2) the repair stage.
3) the late remodelling stage.9
In the inflammatory stage, during the first few hours and days. Inflammatory cells (macrophages, monocytes, lymphocytes, and polymorphonuclear cells) and fibroblasts infiltrate the site.
During the repair stage, fibroblasts begin to lay down a stroma that helps support vascular ingrowth. This weak callus takes 4-6 weeks and needs protection from weight baring and re-injury.
Finally, the callus ossifies, The Remodelling of the bone occurs slowly over months to years and is facilitated by mechanical stress placed on the bone.
Sufficient strength is usually achieved in 3 to 6 months. Soft tissue repair maybe more problematic to bone healing.
Supporting the healing with ultrasound, electrotherapy can significantly influence the healing process.
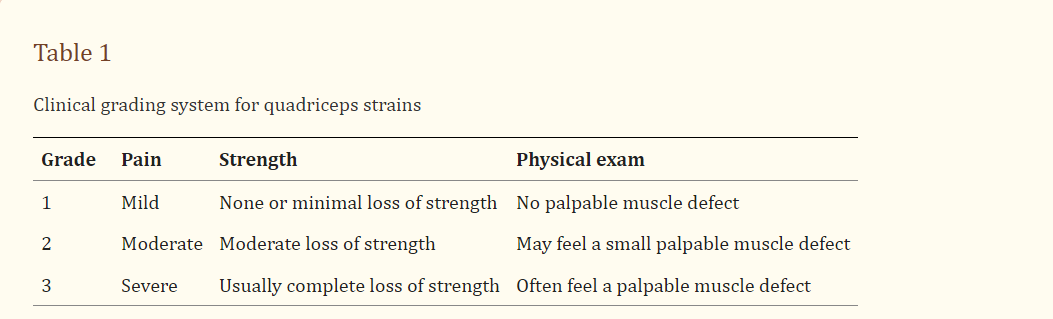
Muscle strain
Grade 1 strains represent minor tearing of muscle fibres with only minimal or no loss in strength. Pain is usually mild to moderate with no palpable defect in the muscle tissue on exam.
Grade 2 strains involve more severe disruption to the muscle fibres with significant pain and loss of strength. A defect in the muscle tissue may sometimes be felt.
Grade 3 strains are a result of complete tearing of the muscle with associated severe pain and complete loss of strength. A palpable defect in the muscle tissue can frequently be felt, especially if examined at onset of injury prior to hematoma formation.
The acute phase of treatment is subsequently followed by an active phase of management once the injured leg is recovering well. This phase usually begins approximately 3–5 days after the initial injury depending on its severity. Stretching, strengthening, range of motion, maintenance of aerobic fitness, proprioceptive exercises, and functional training are the primary components of this phase.
A regeneration process that is similar in most types of muscle injuries, has been observed. However, complete recovery from the injury is compromised due to the development of fibrosis in the second week after the injury. The formed scar tissue always is mechanically inferior and there[1]fore much less able to perform the functions of a normal muscle fibre. It is also more susceptible to reinjury
Three stages are inflammatory phase (1 to 3 days), the repair phase (3 to 4 weeks), and the remodelling phase (3 to 6 months)
Treatment goals are to minimize further damage, relieve pain and spasm, reduce haemorrhage and edema, and promote
Ice should be applied intermittently for 15 to 20 minutes with an interval of 30 to 60 minutes. Longer periods of cold application lead to increased circulation and increased bleeding
Mobilization accelerates capillary ingrowth and promotes the regeneration of muscle fibres.
rest is advised during the first 3 to 7 days to allow the scar tissue to gain strength
Exercises should be started gradually. Isometric training should be followed by isotonic training and isotonic training by isokinetic training once the respective exercises can be performed without pain.
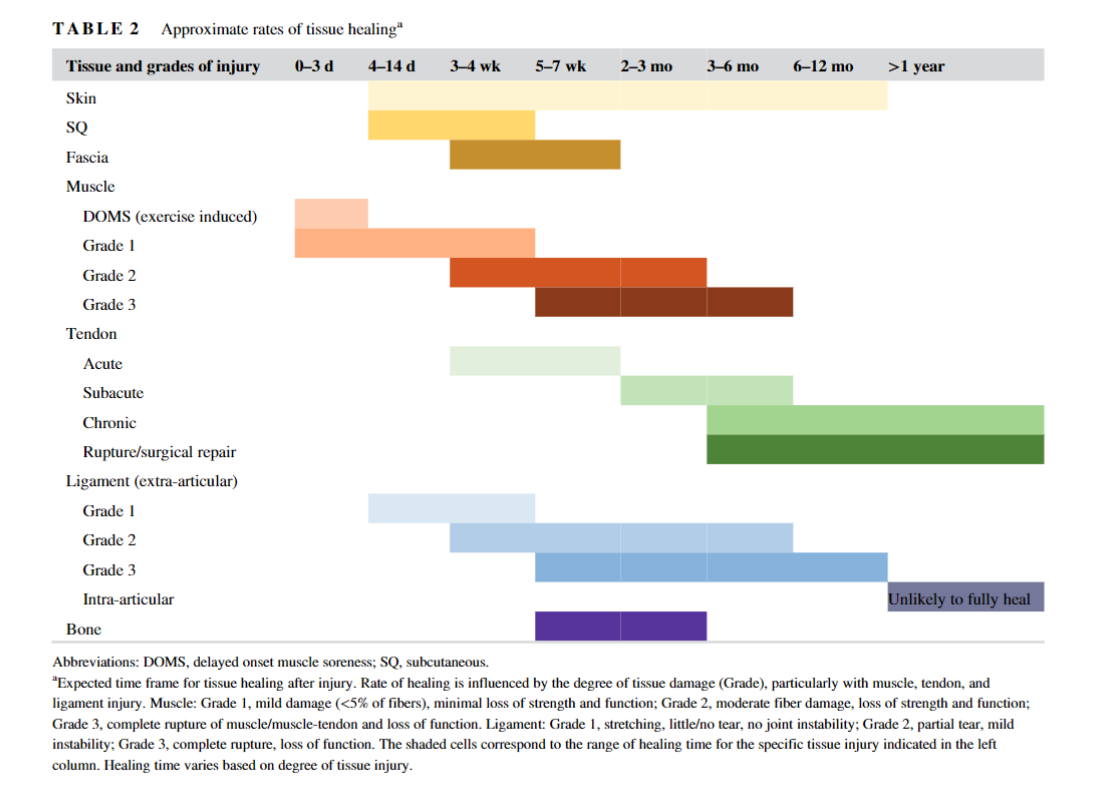
Ligament sprain:
Stress to collagen fibres results in fibre orientation along these specific lines of stress. Specifically, rehabilitation during days 1 through 5 should focus on protection of the injured tissue, then supervised and protected stress may be applied from days 6 to 42.
Early functional rehabilitation of the ankle should include range-of-motion exercises and isometric and isotonic strength-training exercises. In the intermediate stage of rehabilitation, a progression of proprioception-training exercises should be incorporated. Advanced rehabilitation should focus on sport-specific activities to prepare the athlete for return to competition. Although it is important to individualize each rehabilitation program, this well-structured template for ankle rehabilitation can be adapted as needed.
The multifaceted musculoskeletal system offers various ways that proprioception can be affected. Deficits in proprioception have been demonstrated after injury and with articular disease and increasing age. As a joint moves, impulses must arise from muscular, fascial, tendon, and articular receptors. Injury to any or all of these receptors can result in a sensory deficit.
Bulging disc
There are many pathways to a herniated disc including abnormal mechanical work in the form of working posture, exercise and genetic predispositions.
The disc lesions can be classified as Contained or Herniated. The progression of disc degeneration can further be classified as follows: Grade 0: Normal nonleaking nucleus. Grade 1: Annular tearing confined to the inner region of the annulus fibrosis.
Grade 2: In this condition, annular tears have completely disrupted the disc architecture but do not affect the outer contour of the annulus
Grade 3: In this situation, tears have completely disrupted the annulus and the PLL and deformed the contour of the posterior portion of the disc.
Various studies have reported a significant correlation between low back pain and breathing dysfunction. A breathing dysfunction refers to altered breathing patterns which include simple upper chest breathing to hyperventilation. An altered respiration can alter the respiratory chemistry and thus can also influence the tissue oxygenation and electrolyte balance altering body functions including brain and skeletal muscles. Several studies have reported improved function in short term follow-ups with breathing exercises in chronic lower back pain patients.
Depending on the severity it can take between 12 weeks to two years. It is possible to re-injure during healing stage. Some people may need surgery.
Herniated Disc Exercises, 10mins per day.
· Walking
· Bird dog
· Side bridge
· Bridge
· Forward alternating lunge
· Reverse alternating lunge
· Walking lunge
· Cossack squat
Setting the body up for healing:
Bodywork helps to relieve myofascial pain, it is useful to work through fascial adhesions, scar tissue and regain mobility. . It increases blood flow and tissue distensibility and decreases muscle spasm and pain. There is a high recurrence rate unless appropriate exercises are prescribed, with active participation from the patient, to restore flexibility and balance to the muscles. to regain quality of life.
Strengthening and stretching
Hydration
Breath Work, Belly breathing, nose breathing
Appropriate sleep
Good nutrition
Work posture adaptation and accessories
Appropriate mattress and pillow
Lifestyle changes to reduce stress and emotional overload
Daily movement
Emotional support and guidance
A break, holiday, time out.
Finding our joy and carving out time for ourselves.
References:
Baoge, L., Van Den Steen, E. L. K. E., Rimbaut, S., Philips, N., Witvrouw, E., Almqvist, K. F., ... & Vanden Bossche, L. C. (2012). Treatment of skeletal muscle injury: a review. International Scholarly Research Notices, 2012.
Chiarelli, L. Slipped Disc vs. Disc Herniation vs. Disc Bulge By Dr. Liv Chiarelli.
Hoffman, S. J. (2009). Introduction to kinesiology: studying physical activity. Human Kinetics.
Kalfas, I. H. (2001). Principles of bone healing. Neurosurgical focus, 10(4), 1-4.
Kary, J. M. (2010). Diagnosis and management of quadriceps strains and contusions. Current Reviews in Musculoskeletal Medicine, 3(1-4), 26.
Marsh, D. R., & Li, G. (1999). The biology of fracture healing: optimising outcome. British medical bulletin, 55(4), 856-869.
Mascaro, T. B., & Swanson, L. E. (1994). Rehabilitation of the foot and ankle. Orthopedic Clinics of North America, 25(1), 147-160.
Raj, P. P., & FIPP, A. (2008). Intervertebral Disc: Anatomy-Physiology-Pathophysiology-Treatment. Pain Practice, 8(1), 18-44.
Raj, P. P., & FIPP, A. (2008). Intervertebral Disc: Anatomy-Physiology-Pathophysiology-Treatment. Pain Practice, 8(1), 18-44.
Yap, E. C. (2007). Myofascial pain-an overview. Annals-Academy of Medicine Singapore, 36(1), 43.